I used to dread seeing patients with "posterior shoulder pain". In plain English, that's pain in the back of the shoulder. The causes can be vague and difficult to diagnose and treat. One such cause is suprascapular nerve compression. I wasn't the first one to discover suprascapular nerve compression. I didn't invent the surgery to fix it either. However, I've had some really interesting stories treating this fairly rare and strange shoulder problem.
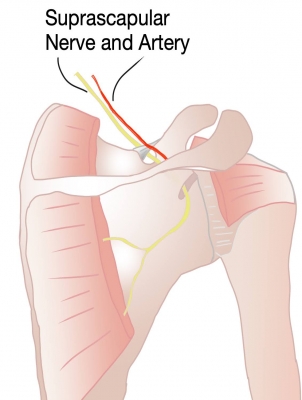
I heard Dr. Laurent LaFosse talk about this problem at the Vumedi Event in San Francisco a few years ago. He called it the "carpal tunnel syndrome of the shoulder". It’s a compression of the suprascapular nerve in the superior scapular notch. If you’ve taken anatomy, you may remember that the suprascapular artery passes over the superior transverse scapular ligament, but the nerve goes under. “Army over, Navy under” the mnemonic goes. This creates a tight spot or a kink point in the nerve leading to pain, usually in the back of the shoulder. JP Warner shared some pearls about treating this problem. Most helpful was the way to diagnose the issue. He showed a diagnostic technique using live X-ray imaging to localize the nerve which sits several centimeters under the skin and muscles of the upper shoulderblade. Once the nerve is located, an injection of lidocaine is used to numb the nerve. If the patient experiences pain relief right after the nerve injection, it confirms the presence of nerve compression.

I have since adopted a similar diagnostic technique using ultrasound imaging because I can do it in the office without using X-rays. Immediately after the lidocaine injection, I ask the patient to try to put their arm in a position that would normally hurt. If the pain is gone (or mostly gone), this establishes the diagnosis of suprascapular nerve compression. In most cases, I mix the lidocaine with some steroid medication that gives a longer lasting pain relief. The patient is advised that the initial pain relief will be short-lived but mimics the relief they’d get from a surgery to release the nerve. The real value of this injection is not so much in treating the pain, but that it helps establish our diagnosis.
Let me share a couple patient stories:
Patient 1:
This patient was in her early 40's. She owned a fish tank cleaning business and came to see me 5 years ago about persistent shoulder pain. She described the pain as "in the front and back" of her shoulder. It prevented her from reaching into a deep tank to scrub the walls. We tried physical therapy and cortisone injections, but she continued to have pain. Eventually, I took her for surgery and performed a bicep tenodesis. Following that surgery, she went to physical therapy and got "a bit better". However, a year later, she continued to have pain "in the top and back" of the shoulder. We were both frustrated and eventually, we decided to go back in to see if I had missed something like impingement of the subscapularis under the coracoid (subcoracoid impingement). I really didn't find much but while I was there, I smoothed the edge of the coracoid. Several months later, she continued to have this vague "crawling pain" in the back of her shoulder. It was about this time that I was getting better at diagnosing suprascapular compression. I tried the injection and the patient told me "it's the first time the shoulder pain has been gone in over 2 years". We finally had our diagnosis.
Armed with this information, we decided to go in for a 3rd surgery. I released the nerve arthroscopically and saw her back a week later. She reported that her pain was gone. She was very happy except for some new onset of weakness in the shoulder. The weakness eventually fully resolved and she returned to full activities at work.
Patient 2:
This patient was in her early 50's. She worked as an attorney. She complained of pain but no weakness. I performed a bicep tenodesis for her shoulder pain but she failed to improve. She was very frustrated but urged me to keep trying to make her shoulder better. We had a radiologist inject her suprascapular nerve with X-ray localization. The patient reported full relief of the pain that had been plaguing her. The numbing medicine subsequently wore off, but we had our diagnosis. I took her back for surgery and released her nerve arthroscopically. She came back to her first postop visit 1 week later reporting full relief of her pain. I saw her again about a month later. With tears in her eyes, she thanked me for curing her shoulder pain and for "not giving up on me".
As of this writing, I have performed 15 suprascapular nerve releases. One was in a patient with a massive rotator cuff and I didn’t do a diagnostic injection prior to surgery. In the remaining 14, I did a diagnostic injection in all of them. Thankfully, I have been more keen to look for the problem and have not had to do any "redos" as I did in these early 2 patients. Aside from patient 1 who had a temporary neuropraxia, I have not had any nerve injuries. The 14 patients with isolated suprascapular nerve compressions have all had full relief of their pain. In most cases, the pain relief was noticeable by the first postop visit.
Here's a video of how I release the supra-scapular nerve endoscopically.